 | You Don't Know What |
A newer 2020 (with a COVID19 preface) version of this post can be viewed if you CLICK HERE!
I have updated this post several times, and it has been very helpful to many in the myeloma patient community. I believe one key area which could have the greatest impact on patient survival is the improved dissemination of the myeloma specialist approved best treatments for each individual patient. The 20% of myeloma patients who see a myeloma specialist or consult with one, are provided with the best current treatment knowledge, but this leaves the remaining 80% underserved. How then do we make this happen?
One thing has become very clear to me, the pace of change and progress for myeloma has become exponential. This is a very good thing! We have had 5 drugs approved for myeloma since 2015 (two are new classes of drugs). In addition, new targeted treatments like CAR T and ADC(Antibody Drug Conjugates) have exploded with just 3 myeloma CAR T ASH(American Society of Hematology) abstracts listed in 2009, and in 2018 ASH lists 104 myeloma CAR T abstracts or 35 times as many.
As a patient advocate I find it nearly impossible to keep up with the avalanche of new data. I can not see how anyone but a skilled myeloma specialist can keep up to date with this rapid pace of change. But Dr. Lonial, a world class myeloma specialist from Emory University, says it best: CLICK HERE to view his advice.
Most myeloma specialists, and most knowledgeable patients and advocates believe this to be critical. However, even with the need for a specialist input so obvious, 80% of patients do not see a myeloma specialist or obtain their input for a treatment plan. I have written about this in a blog post titled, "The Myeloma Conundrum! Myeloma Specialists Do Not Grow On Trees!" What this highlights is myeloma specialists are already working at their maximum, so even if the 80% wanted to see a specialist, there is just not enough specialists to handle all of the patients. The solution identified in this post is to put expert information and guidance into the hands of the local hematologists, oncologists, and patients will receive expert input and achieve much better outcomes.
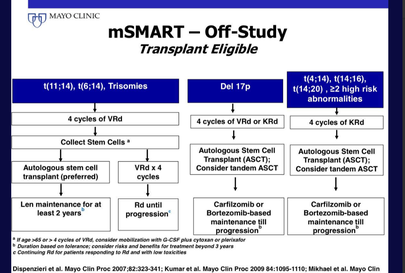
Mayo Clinic has developed the mSmart program. This program provides a template that doctors can follow to provide care outlined designed and developed by some of the very best minds in myeloma research and treatment. You can go to the mSmart site if you CLICK HERE. A sample of the information presented on the site is shown to the left.
Currently under development, Dr. Fonseca of Mayo, Phoenix and the Myeloma Crowd have put together what I would call the next step in the process to make expert advice individualized, and in a manner patients can use and understand. It was designed by myeloma experts, myeloma patients and is called The Health Tree. You can learn more about the program and find your best individualized treatment if you CLICK HERE. Until there is a massive increase in the number of myeloma specialists, these two sources are your best bet for the underserved 80%.
In the last two years, the average life expectancy has gone from 4 years to 5.5. years, according to The SEER(Surveillance, Epidemiology, and End Results) data for multiple myeloma published in April of 2018 by the National Cancer Institute. This is outstanding progress in that life expectancy had been stagnant at 4 years for 5 consecutive years. Some patients beat the odds and live 10 to 20 years or more. When I was first diagnosed, the data for a person with dialysis-dependent kidney failure was just 3 months, and the average for myeloma patients overall was about 3 years. Now, I am beyond thankful to be a nearly 13 year survivor. I believe there are three critical components to beating the odds: Part one is early diagnosis and treatment before end organ damage. Part two is disease dependent, or the hand that you were dealt. Part three is related to the level of care that is available to you. For more information on survival rates and life expectancy CLICK HERE.
Part 1 - Early Diagnosis and Treatment
If you are lucky enough to have a general practitioner who picks up high protein in the blood and finds the disease early while it is smoldering, or stage one, you have won the Myeloma Lottery. Life expectancy of stage one disease is 3 times greater than if you have been found in stage three. Treatment guidelines were published in November of 2014 with the express purpose of finding and treating the disease before it has progressed and causes end organ failure. A National Institute of health article states the intent of this clearly; "The concept of initiating therapy after end organ damage is analogous to initiating treatment after the development of metastatic cancer in solid tumors. Indeed, screening, early detection and intervention have played a large part in the major curative advances that have been achieved in solid tumors whereas metastatic cancer remains incurable in these same malignancies. It is, therefore, not surprising that MM remains incurable, in spite of all the advances in therapeutic interventions. Could it be because we are waiting too long – until metastatic myeloma occurs – to treat our patients? In such a condition, watchful waiting may actually be more harmful to the patient than early intervention." To read the whole article CLICK HERE! If you are one of the lucky ones who are found in the early stages of active myeloma or smoldering myeloma, you will have the luxury of time to understand the treatment options, find a myeloma specialist (a must), and plan to confront your disease before permanent end organ damage. Dr. Rajkumar of Mayo Clinic did a wonderful job of explaining the new criteria for myeloma diagnosis, and you can read it if you CLICK HERE. Dr. Irene Ghobrial is doing some great work to follow MGUS and smoldering stages of the disease, to develop treatments to cure, or at least prevent end organ damage. CLICK HERE to view a myeloma crowd interview with Dr. Ghobrial on the subject. Just as a note, the country of Iceland is testing all of its adult population over 40 to screen for MGUS, Smoldering, and active myeloma. They call it iStopMM, a clinical trial supported by the IMF(International Myeloma Foundation). This is a future I pray we will all see where we could cost effectively find MM early and treat it before end organ damage. CLICK HERE or HERE to learn more about iStopMM.
Unfortunately, Myeloma UK has reported that 1 in 5 myeloma patients die within the first two months of diagnosis, and that it takes nearly a year from the first symptoms to diagnosis for 25% of newly diagnosed patients. Dr. Morgan of UAMS said it best when he outlined his thoughts on the subject of awareness and delayed diagnosis. He believes the fact that it takes 3 to 6 months and more often 6 months from first symptoms to diagnosis is a bit of a scandal. To make real inroads in the myeloma we need to get it diagnosed early before we have organ involvement. We need to make family doctors and family practitioners more aware of the disease. They should do M spike and light chain tests on patients. This makes a lot of sense to Dr. Morgan. It is really tragic when patients develop renal failure when awareness of myeloma by a General Practitioner might have allowed the patient to get a consult or treatment from a myeloma specialist. A myeloma specialist is critical to a patient's long term care and survival. It is a disease that does not come on overnight but is years in the making. Patient organizations can make a difference. He believes the future of Myeloma will be to get earlier diagnosis, safe treatments, chemo prevention strategy, regular screening for para protein, and early intervention.
I have kidney damage, a good friend of mine has debilitating bone pain, others collapsed vertebrae, one suffers from a myeloma caused stroke, and many have died from delayed diagnosis. All of which might have been prevented with a simple test of light chains and M spike costing under $150 without insurance, and no cost if covered by insurance and referred by a General Practitioner. It is what could be!
Part 2 - Disease Dependent
Some people are just plain lucky and are given a form of myeloma that is not that aggressive. In other words they have myeloma, but it happens to be smoldering myeloma. This form of the disease can be present in the patient but not show any outward symptoms. It can remain in this mode for 5, 10, or even 20 years.
The age of the patient is very important, in that you are 2 times more likely to survive if you were diagnosed at 49 years of age or less. The average age of the typical myeloma patient is 70. You can read more on this subject if you CLICK HERE.
Some people may have an active disease but do not have any of the negative prognostic indicators. These indicators include, but are not limited to, deletion of chromosome 17p and translocation of 4;14 or 14;16 or 14;20. Your myeloma specialist will run the FISH test or other genetic tests like GEP(gene expression profiling) to determine if you have any of these negative prognostic indicators. If you are considered high risk(15% of patients) , the life expectancy is less than half of the current average, or just 2 years. You can read more about high risk multiple myeloma if you CLICK HERE.
The sensitivity of the disease to treatment is also important. My myeloma seemed to be very sensitive to the combination of Cytoxan, Thalamid and Dexamethasone, a treatment that put me into remission very quickly. Some people might have the same experience with Revlimid, Velcade, or Dex, or any combination of these drugs. If the disease comes back, as it often does, the re-application of the same regimen may continue to work for years. I know one patient who has taken Thalomid for years as his only treatment and remains in remission.
And of course if the average is 5.5 years, half of the people will invariably beat the average.
Part 3 - Quality of Care
There are some elements that you may or may not have much control over, the first of which is the availability of insurance. If you do not have insurance or have no access to care, the average life expectancy is less than one year. However, Medicare has a Compassionate Allowance Program where you can be approved in less than two weeks if you go to your local office and can show that you will not live without care. To see the program CLICK HERE. The Affordable Care Act may provide an option for the 15% who are not insured, and Medicare, Medicaid, and drug company assistance programs are also available. In addition, there are other programs which can provide assistance listed on the bottom of the home page, to view CLICK HERE.
Multiple Myeloma is a rare blood cancer, so many hematologist/oncologists may not see one patient in a year. As a result not all oncologists or hematologists are the same. However, some are very skilled and experienced with Multiple Myeloma and have treated many myeloma patients. The data shows these myeloma specialists provide an average life expectancy of 10+ years or more, compared to the average which is at 5.5 years.
For a listing of these exceptional specialists CLICK HERE or for a more extensive list without survival history just CLICK HERE. I chose to get my 2 SCT(stem cell transplants) at University of Arkansas for Medical Sciences, UAMS, which has a myeloma program called MIRT, Myeloma Institute of Research and Therapy. At the time they had over 10,000 transplants under their belt, and as a result they were expert at the process, and knew what could go wrong and had a plan in place to get you through any potential complications. I have found from my work on this site that centers like Mayo, Dr. Hari(Medical College of Wisconsin), UAMS, or Dr. Berenson's (IMBCR) have very different approaches to treatment, but because they are expert in what they do, they have similar results. You would choose a brain surgeon over any other surgeon if you had a brain tumor, why would you not do the same for myeloma? Find out how to find a myeloma specialist by CLICKING HERE or CLICKING HERE.
Myeloma specialists have access to drugs that other oncologists do not. Because they are the thought leaders, they are involved in clinical trials, and can obtain some drugs through other programs that lesser known oncologists do not have access to. Worse yet, oncologists who are not myeloma specialists may not even know that some of these drugs even exist. For example, some of the well connected specialists have access to drugs or treatments like CAR T, MILs, Venetoclax or Selinexor which are not approved treatments. But these experts can get approval for initial therapy through clinical trials or other programs. Or some specialists can use drugs that are only approved for relapse or secondary therapy options (Daratumumab, Ixazomib, Krypolis and Pomalyst), and obtain approval to use them for newly diagnosed patients. They also have access to the best clinical trials like KRDD(Krypolis, Revlimid, Darzalex, & dexamethasone) for first line therapy which provides a response in 100 percent of patients. When you run out of options with the currently approved drugs, they can provide access to those that have done great in clinical trial, but are not currently available to the general public. Because you need a significant infrastructure to conduct clinical trials at your facility and they cost the facility $15,000 per patient, few local oncologists have access to clinical trials. Sometimes it is who you know!
Myeloma patients seldom die from myeloma, they die from the complications from myeloma. The number one complication is pneumonia, and others include infections, kidney failure, anemia, etc. This, therefore, brings me to the realization that supportive care for the treatment of the many complications of this disease may just be as important as the cancer treatment itself. Or a great Defense(supportive care) is as important as the Offense(cancer therapy). MD Anderson and Mayo Clinic emphasize supportive care in their programs, UAMS actually has a Director of Supportive Care in their myeloma program, Dr. Elias Anaissie, now a Medical Director at Clinical Trial and Consulting Services (CTI). has an extensive background in supportive care. Dr. Anaissie has published a well written example of an exceptional supportive care model. You can read this publication if you CLICK HERE. To read my blog post on supportive care CLICK HERE.
I also think the quality of care that you receive can be affected by the knowledge of the patient, and this can be obtained by doing your research on finding the best approaches to care by looking at the work of the best myeloma specialists on-line, and by going to great sites as listed in the Resource Section of www.myelomasurvival.com. To find out how to get educated about multiple myeloma CLICK HERE. In addition, joining a support group of the International Myeloma Foundation or the LLS (Leukemia, Lymphoma, and Myeloma Society) will provide more great information to improve your life expectancy. I have found that the average life expectancy of most of these support groups far out-performs the average. Knowledge is power! Additional information on the benefits of support group membership can be found if you CLICK HERE.
With 30,000 new cases of multiple myeloma in the USA, we can estimate the total number of patients in just the USA at 165,000. If we can move the average life expectancy from 5.5 years to 11 years by having myeloma specialists guide your care, we could save 165,000 times 5.5, or 907,500 years of LIFE. Many times more if we include the entire world. You all can help by getting this message out to the myeloma patient community through Facebook and Twitter. You may know someone who has myeloma or may have a friend or family member that can be helped by this information. With your help we can "SAVE LIFE"!
Good luck and God Bless your Myeloma Journey/ [email protected]
For more information on multiple myeloma CLICK HERE and you can follow me on twitter at: https://twitter.com/grpetersen1
I have updated this post several times, and it has been very helpful to many in the myeloma patient community. I believe one key area which could have the greatest impact on patient survival is the improved dissemination of the myeloma specialist approved best treatments for each individual patient. The 20% of myeloma patients who see a myeloma specialist or consult with one, are provided with the best current treatment knowledge, but this leaves the remaining 80% underserved. How then do we make this happen?
One thing has become very clear to me, the pace of change and progress for myeloma has become exponential. This is a very good thing! We have had 5 drugs approved for myeloma since 2015 (two are new classes of drugs). In addition, new targeted treatments like CAR T and ADC(Antibody Drug Conjugates) have exploded with just 3 myeloma CAR T ASH(American Society of Hematology) abstracts listed in 2009, and in 2018 ASH lists 104 myeloma CAR T abstracts or 35 times as many.
As a patient advocate I find it nearly impossible to keep up with the avalanche of new data. I can not see how anyone but a skilled myeloma specialist can keep up to date with this rapid pace of change. But Dr. Lonial, a world class myeloma specialist from Emory University, says it best: CLICK HERE to view his advice.
Most myeloma specialists, and most knowledgeable patients and advocates believe this to be critical. However, even with the need for a specialist input so obvious, 80% of patients do not see a myeloma specialist or obtain their input for a treatment plan. I have written about this in a blog post titled, "The Myeloma Conundrum! Myeloma Specialists Do Not Grow On Trees!" What this highlights is myeloma specialists are already working at their maximum, so even if the 80% wanted to see a specialist, there is just not enough specialists to handle all of the patients. The solution identified in this post is to put expert information and guidance into the hands of the local hematologists, oncologists, and patients will receive expert input and achieve much better outcomes.
Mayo Clinic has developed the mSmart program. This program provides a template that doctors can follow to provide care outlined designed and developed by some of the very best minds in myeloma research and treatment. You can go to the mSmart site if you CLICK HERE. A sample of the information presented on the site is shown to the left.
Currently under development, Dr. Fonseca of Mayo, Phoenix and the Myeloma Crowd have put together what I would call the next step in the process to make expert advice individualized, and in a manner patients can use and understand. It was designed by myeloma experts, myeloma patients and is called The Health Tree. You can learn more about the program and find your best individualized treatment if you CLICK HERE. Until there is a massive increase in the number of myeloma specialists, these two sources are your best bet for the underserved 80%.
In the last two years, the average life expectancy has gone from 4 years to 5.5. years, according to The SEER(Surveillance, Epidemiology, and End Results) data for multiple myeloma published in April of 2018 by the National Cancer Institute. This is outstanding progress in that life expectancy had been stagnant at 4 years for 5 consecutive years. Some patients beat the odds and live 10 to 20 years or more. When I was first diagnosed, the data for a person with dialysis-dependent kidney failure was just 3 months, and the average for myeloma patients overall was about 3 years. Now, I am beyond thankful to be a nearly 13 year survivor. I believe there are three critical components to beating the odds: Part one is early diagnosis and treatment before end organ damage. Part two is disease dependent, or the hand that you were dealt. Part three is related to the level of care that is available to you. For more information on survival rates and life expectancy CLICK HERE.
Part 1 - Early Diagnosis and Treatment
If you are lucky enough to have a general practitioner who picks up high protein in the blood and finds the disease early while it is smoldering, or stage one, you have won the Myeloma Lottery. Life expectancy of stage one disease is 3 times greater than if you have been found in stage three. Treatment guidelines were published in November of 2014 with the express purpose of finding and treating the disease before it has progressed and causes end organ failure. A National Institute of health article states the intent of this clearly; "The concept of initiating therapy after end organ damage is analogous to initiating treatment after the development of metastatic cancer in solid tumors. Indeed, screening, early detection and intervention have played a large part in the major curative advances that have been achieved in solid tumors whereas metastatic cancer remains incurable in these same malignancies. It is, therefore, not surprising that MM remains incurable, in spite of all the advances in therapeutic interventions. Could it be because we are waiting too long – until metastatic myeloma occurs – to treat our patients? In such a condition, watchful waiting may actually be more harmful to the patient than early intervention." To read the whole article CLICK HERE! If you are one of the lucky ones who are found in the early stages of active myeloma or smoldering myeloma, you will have the luxury of time to understand the treatment options, find a myeloma specialist (a must), and plan to confront your disease before permanent end organ damage. Dr. Rajkumar of Mayo Clinic did a wonderful job of explaining the new criteria for myeloma diagnosis, and you can read it if you CLICK HERE. Dr. Irene Ghobrial is doing some great work to follow MGUS and smoldering stages of the disease, to develop treatments to cure, or at least prevent end organ damage. CLICK HERE to view a myeloma crowd interview with Dr. Ghobrial on the subject. Just as a note, the country of Iceland is testing all of its adult population over 40 to screen for MGUS, Smoldering, and active myeloma. They call it iStopMM, a clinical trial supported by the IMF(International Myeloma Foundation). This is a future I pray we will all see where we could cost effectively find MM early and treat it before end organ damage. CLICK HERE or HERE to learn more about iStopMM.
Unfortunately, Myeloma UK has reported that 1 in 5 myeloma patients die within the first two months of diagnosis, and that it takes nearly a year from the first symptoms to diagnosis for 25% of newly diagnosed patients. Dr. Morgan of UAMS said it best when he outlined his thoughts on the subject of awareness and delayed diagnosis. He believes the fact that it takes 3 to 6 months and more often 6 months from first symptoms to diagnosis is a bit of a scandal. To make real inroads in the myeloma we need to get it diagnosed early before we have organ involvement. We need to make family doctors and family practitioners more aware of the disease. They should do M spike and light chain tests on patients. This makes a lot of sense to Dr. Morgan. It is really tragic when patients develop renal failure when awareness of myeloma by a General Practitioner might have allowed the patient to get a consult or treatment from a myeloma specialist. A myeloma specialist is critical to a patient's long term care and survival. It is a disease that does not come on overnight but is years in the making. Patient organizations can make a difference. He believes the future of Myeloma will be to get earlier diagnosis, safe treatments, chemo prevention strategy, regular screening for para protein, and early intervention.
I have kidney damage, a good friend of mine has debilitating bone pain, others collapsed vertebrae, one suffers from a myeloma caused stroke, and many have died from delayed diagnosis. All of which might have been prevented with a simple test of light chains and M spike costing under $150 without insurance, and no cost if covered by insurance and referred by a General Practitioner. It is what could be!
Part 2 - Disease Dependent
Some people are just plain lucky and are given a form of myeloma that is not that aggressive. In other words they have myeloma, but it happens to be smoldering myeloma. This form of the disease can be present in the patient but not show any outward symptoms. It can remain in this mode for 5, 10, or even 20 years.
The age of the patient is very important, in that you are 2 times more likely to survive if you were diagnosed at 49 years of age or less. The average age of the typical myeloma patient is 70. You can read more on this subject if you CLICK HERE.
Some people may have an active disease but do not have any of the negative prognostic indicators. These indicators include, but are not limited to, deletion of chromosome 17p and translocation of 4;14 or 14;16 or 14;20. Your myeloma specialist will run the FISH test or other genetic tests like GEP(gene expression profiling) to determine if you have any of these negative prognostic indicators. If you are considered high risk(15% of patients) , the life expectancy is less than half of the current average, or just 2 years. You can read more about high risk multiple myeloma if you CLICK HERE.
The sensitivity of the disease to treatment is also important. My myeloma seemed to be very sensitive to the combination of Cytoxan, Thalamid and Dexamethasone, a treatment that put me into remission very quickly. Some people might have the same experience with Revlimid, Velcade, or Dex, or any combination of these drugs. If the disease comes back, as it often does, the re-application of the same regimen may continue to work for years. I know one patient who has taken Thalomid for years as his only treatment and remains in remission.
And of course if the average is 5.5 years, half of the people will invariably beat the average.
Part 3 - Quality of Care
There are some elements that you may or may not have much control over, the first of which is the availability of insurance. If you do not have insurance or have no access to care, the average life expectancy is less than one year. However, Medicare has a Compassionate Allowance Program where you can be approved in less than two weeks if you go to your local office and can show that you will not live without care. To see the program CLICK HERE. The Affordable Care Act may provide an option for the 15% who are not insured, and Medicare, Medicaid, and drug company assistance programs are also available. In addition, there are other programs which can provide assistance listed on the bottom of the home page, to view CLICK HERE.
Multiple Myeloma is a rare blood cancer, so many hematologist/oncologists may not see one patient in a year. As a result not all oncologists or hematologists are the same. However, some are very skilled and experienced with Multiple Myeloma and have treated many myeloma patients. The data shows these myeloma specialists provide an average life expectancy of 10+ years or more, compared to the average which is at 5.5 years.
For a listing of these exceptional specialists CLICK HERE or for a more extensive list without survival history just CLICK HERE. I chose to get my 2 SCT(stem cell transplants) at University of Arkansas for Medical Sciences, UAMS, which has a myeloma program called MIRT, Myeloma Institute of Research and Therapy. At the time they had over 10,000 transplants under their belt, and as a result they were expert at the process, and knew what could go wrong and had a plan in place to get you through any potential complications. I have found from my work on this site that centers like Mayo, Dr. Hari(Medical College of Wisconsin), UAMS, or Dr. Berenson's (IMBCR) have very different approaches to treatment, but because they are expert in what they do, they have similar results. You would choose a brain surgeon over any other surgeon if you had a brain tumor, why would you not do the same for myeloma? Find out how to find a myeloma specialist by CLICKING HERE or CLICKING HERE.
Myeloma specialists have access to drugs that other oncologists do not. Because they are the thought leaders, they are involved in clinical trials, and can obtain some drugs through other programs that lesser known oncologists do not have access to. Worse yet, oncologists who are not myeloma specialists may not even know that some of these drugs even exist. For example, some of the well connected specialists have access to drugs or treatments like CAR T, MILs, Venetoclax or Selinexor which are not approved treatments. But these experts can get approval for initial therapy through clinical trials or other programs. Or some specialists can use drugs that are only approved for relapse or secondary therapy options (Daratumumab, Ixazomib, Krypolis and Pomalyst), and obtain approval to use them for newly diagnosed patients. They also have access to the best clinical trials like KRDD(Krypolis, Revlimid, Darzalex, & dexamethasone) for first line therapy which provides a response in 100 percent of patients. When you run out of options with the currently approved drugs, they can provide access to those that have done great in clinical trial, but are not currently available to the general public. Because you need a significant infrastructure to conduct clinical trials at your facility and they cost the facility $15,000 per patient, few local oncologists have access to clinical trials. Sometimes it is who you know!
Myeloma patients seldom die from myeloma, they die from the complications from myeloma. The number one complication is pneumonia, and others include infections, kidney failure, anemia, etc. This, therefore, brings me to the realization that supportive care for the treatment of the many complications of this disease may just be as important as the cancer treatment itself. Or a great Defense(supportive care) is as important as the Offense(cancer therapy). MD Anderson and Mayo Clinic emphasize supportive care in their programs, UAMS actually has a Director of Supportive Care in their myeloma program, Dr. Elias Anaissie, now a Medical Director at Clinical Trial and Consulting Services (CTI). has an extensive background in supportive care. Dr. Anaissie has published a well written example of an exceptional supportive care model. You can read this publication if you CLICK HERE. To read my blog post on supportive care CLICK HERE.
I also think the quality of care that you receive can be affected by the knowledge of the patient, and this can be obtained by doing your research on finding the best approaches to care by looking at the work of the best myeloma specialists on-line, and by going to great sites as listed in the Resource Section of www.myelomasurvival.com. To find out how to get educated about multiple myeloma CLICK HERE. In addition, joining a support group of the International Myeloma Foundation or the LLS (Leukemia, Lymphoma, and Myeloma Society) will provide more great information to improve your life expectancy. I have found that the average life expectancy of most of these support groups far out-performs the average. Knowledge is power! Additional information on the benefits of support group membership can be found if you CLICK HERE.
With 30,000 new cases of multiple myeloma in the USA, we can estimate the total number of patients in just the USA at 165,000. If we can move the average life expectancy from 5.5 years to 11 years by having myeloma specialists guide your care, we could save 165,000 times 5.5, or 907,500 years of LIFE. Many times more if we include the entire world. You all can help by getting this message out to the myeloma patient community through Facebook and Twitter. You may know someone who has myeloma or may have a friend or family member that can be helped by this information. With your help we can "SAVE LIFE"!
Good luck and God Bless your Myeloma Journey/ [email protected]
For more information on multiple myeloma CLICK HERE and you can follow me on twitter at: https://twitter.com/grpetersen1
 RSS Feed
RSS Feed